Medicare Advantage Overpayments: Why Coding Intensity is Costing Taxpayers Billions
Discover how Medicare Advantage coding practices drive up federal spending, creating a $76 billion gap between private plans and traditional Medicare costs.
The Financial Impact of Risk Adjustment
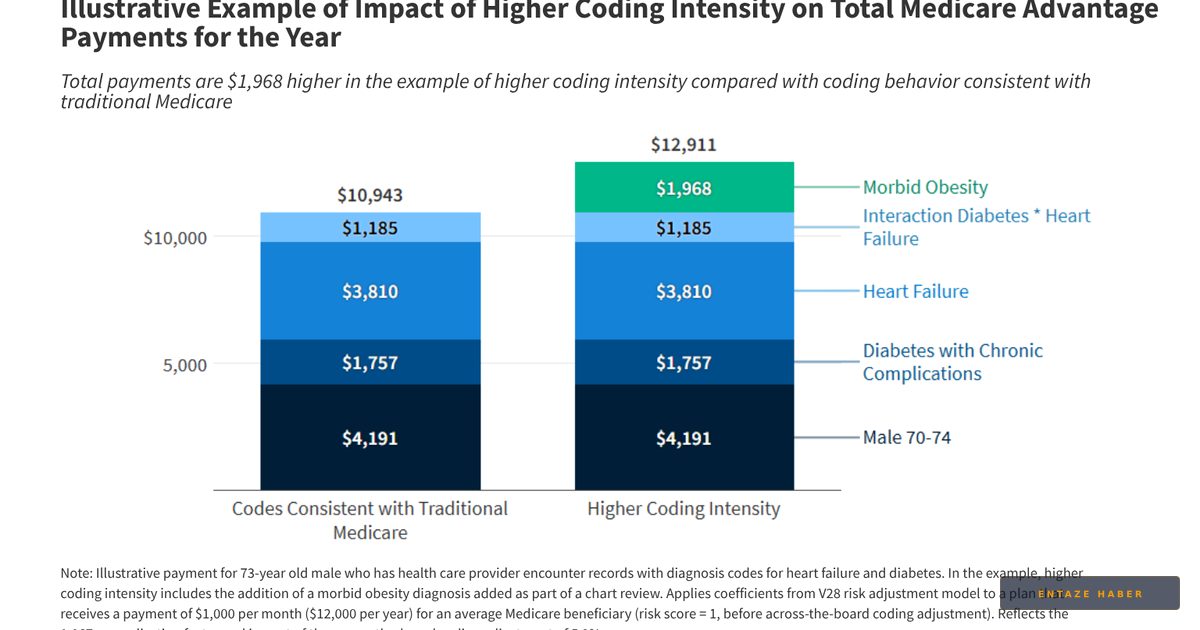
The federal government faces growing pressure to address how Medicare Advantage (MA) plans are compensated. These private insurers receive capitated monthly payments, which are risk-adjusted based on the health status of their enrollees. By reporting specific diagnosis codes to the Centers for Medicare & Medicaid Services (CMS), plans secure higher payments for patients with complex medical needs. While this system aims to ensure adequate funding for high-cost enrollees, it creates a perverse incentive for insurers to aggressively capture every possible diagnosis code. This practice, known as coding intensity, leads to inflated risk scores and higher federal expenditures compared to traditional Medicare.

Traditional Medicare vs. Private Plan Disparities
Unlike private MA plans, traditional Medicare does not reward providers for maximizing diagnosis documentation; billing is tied strictly to services rendered. This fundamental difference creates a structural imbalance. Because MA plans utilize health risk assessments and chart reviews—often powered by AI—to identify additional conditions not always treated during the year, their enrollees appear sicker than they would under traditional fee-for-service models. The Medicare Payment Advisory Commission (MedPAC) estimates that in 2026, total payments to MA plans will exceed traditional Medicare spending by $76 billion, with $28 billion directly attributed to these coding discrepancies.

CMS Policy Shifts and Future Oversight
CMS is actively moving to tighten payment accuracy. The 2027 rate notice introduces stricter rules regarding how diagnoses are considered, specifically limiting the impact of "unlinked" chart reviews where codes are added without a corresponding patient-provider encounter. Furthermore, the implementation of the V28 risk adjustment model represents a significant effort to recalibrate how chronic conditions influence payment. While these measures aim to reduce the uncorrected coding intensity—which MedPAC projects at 4% for 2026—the ongoing challenge remains to align private plan incentives with actual patient health outcomes.
Recent Developments
The landscape of federal health insurance is shifting as regulators roll out new policies to curb excessive spending in private plans. This breaking news reflects the latest updates from CMS regarding risk adjustment methodologies and their impact on future fiscal years. You can follow all developments instantly on MedicareTicker.com.
Related Topics
🔹 Medicare Advantage 🔹 CMS Payment Policy 🔹 Risk Adjustment 🔹 Healthcare Finance 🔹 MedPAC Reports 🔹 Federal Health Spending
Comparisons News
This category provides a critical look at how different insurance models operate within the U.S. healthcare system. MedicareTicker.com offers live coverage and the latest updates on these comparisons, ensuring readers stay informed on breaking news regarding public and private health coverage.
Frequently Asked Questions
What is coding intensity?
Coding intensity refers to the variation in how health conditions are documented between different insurance models. It specifically highlights how private MA plans often generate higher risk scores than traditional Medicare by documenting more conditions.
Why does coding intensity increase federal costs?
Because risk scores determine monthly payments, insurers have a financial incentive to record as many diagnoses as possible. This leads to higher per-enrollee payments from the government, even when those conditions do not require additional care.
What are unlinked chart reviews?
These are reviews of medical records conducted by insurers to find additional diagnosis codes. If these codes are not linked to an actual clinical encounter with a physician, they are considered 'unlinked' and are now being restricted by new CMS policies.